
Brain and spine operations are typically performed with patients asleep. While these surgeries are intricately executed by surgeons with highly specialized training, the nervous structures commonly are manipulated. Techniques for examining the nervous system are limited in the asleep patient. To ensure temporary or permanent damage does not occur, intraoperative monitoring (IOM) is commonly performed. The goal of IOM is to identify brain, spinal cord, and nerve irritation/injury at a time when the surgeon can take steps to reduce or reverse it and identify the injury in a way that allows the surgeon to complete the procedure without further injury.
IOM Tests
Three standard IOM tests are commonly used. Somatosensory evoked potential (SSEP) monitoring assesses the sensory pathways in the brain and spinal cord. Generally speaking, SSEPs assess if the patient will maintain sensation, or “feeling.” Diminished SSEPs could result in numbness, loss of fine touch or coordination problems. The second IOM test is motor evoked potential (MEP) monitoring. MEPs assess the motor function in the brain and spinal cord, or ability for the patient to move. Diminished MEPs could result in weakness or paralysis. The third IOM test is electromyography (EMG). When a nerve is irritated, it causes an electrical change in the associated muscles. EMG changes, unfortunately, are a poor predictor of actual postoperative dysfunction.
One of the greatest challenges in IOM is that the prediction of neurologic deficit is not perfect. It still is possible for the recordings to be normal during surgery, but the patient wakes up with a neurologic deficit including weakness, numbness or pain. On the other hand, it’s possible for the IOM to mistakenly change during a procedure without any resultant injury to the nerves. This can occur even just from type/amount of anesthesia medications, changes in body temperature or changes in blood pressure. Despite these pitfalls in IOM, it tends to be accurate and makes most procedures safer. Most patients would agree that it’s worthwhile to use IOM if it potentially prevents them from waking from surgery with unexpected weakness, numbness or pain.
How IOM Tests Work
IOM requires extra personnel and equipment to be used in surgery. Small needles are placed in the patient’s skin (sometimes patients notice little areas of bruising on their extremities) and electrodes may be placed on the scalp. The cords from these needles and electrodes attach to a complex transducer and then to a computer. An IOM technician sits in the operating room during the surgery to both place the needles/electrodes after the patient is asleep and then verify recordings are correctly being transmitted to the computer. If there are any IOM changes, this technician can help troubleshoot and make sure the connections are correct and address any changes required in anesthesia or patient temperature/blood pressure. An additional physician then remotely interprets the results during the procedure. Even though this physician is not physically present in the operating room, they are in a separate location constantly monitoring the IOM recordings and communicating with the technician, surgeon, and anesthesiologist.
The Cost of IOM
Without question, the cost of IOM is extra and not included in the charges by the surgeon, anesthesiologist or hospital. As can be expected from the fact that IOM requires a technician, a physician, and complex equipment, these costs can be substantial. Unfortunately, and for reasons beyond the scope of this blog, absolutely no insurance company (commercial, Medicare or Medicaid) pays for IOM “in-network.” Fees from insurance companies occur in the form of “in-network” and “out-of-network” charges. Depending on the individual insurance contract, the cheapest option for the patient tends to be “in-network” as their typical deductible or co-pay applies. Some insurance companies partially pay for or address “out-of-network” costs, but sometimes “out-of-network” costs are solely placed on the patient. These can be up to 50 times higher than an “in-network” charge. Therefore, on occasion, a patient may receive an “out-of-network” bill that is substantial. Understandably, this is concerning to the uninformed patient if the charge is unexpected. This has led to numerous recent local news stories describing large bills (occasionally $100,000). If you as a patient ever receive a large “out-of-network” bill for IOM, it’s important to verify it’s a bill versus a description of the charge. Next, you should call your insurance company to discuss your responsibility to pay. In some instances, this IOM bill can be negotiated considerably.


Multiple recent Colorado news reports have indicated the IOM bills are “unjustified.” This is only partially correct. IOM is without question an integral component to certain brain and spine surgeries and is worthy of being charged. It is not medically unnecessary. Furthermore, insurance companies need to address this cost of surgery and negotiate an “in-network” rate of some sort. It’s simply not fair for the insurance company to place the cost of an integral component of surgery solely on the patient. However, the controversy arises in that many surgeons themselves are part owners in these IOM companies, and some IOM companies are intentionally and irresponsibly grossly overcharging because the charges are “out-of-network” and sometimes get paid in full.
Owners of IOM Companies
Certain surgeons are either part-owners in the IOM company, receive a kickback for using the IOM, or charge a fee to independently interpret the IOM recordings after the surgery. If the surgeon is independently interpreting the recordings, then they are justified in receiving payment for this extra service. If the surgeon is just a part-owner in the company or receiving a kickback for using a certain company, then payment is unjustified.
In a recent case reported at a local Colorado hospital, a check of $169,600 was paid in full to an IOM company. This is unusual. IOM has been studied in regard to its cost-effectiveness. A single level cervical fusion on average increases cost of the surgery by 16.2 percent. A single level lumbar fusion on average increases cost by 7.8 percent. This on average adds a few thousand dollars to a surgery, not over $100,000. It’s absurd for some IOM companies to charge these amounts.

Discuss IOM with Your Surgeon and Insurance Company
In considering brain or spine surgery, it’s important to discuss IOM with your surgeon and your insurance company. Most likely IOM will be used. Your insurance company may be able to estimate the cost to you based on the type of surgery being performed. However, your surgeon should also indicate if they are part-owner in the IOM company or if they receive a kickback. Your surgeon should also provide you the name of the IOM company, so you can verify their reputation. The surgeon at Rocky Mountain Brain & Spine Institute has absolutely no ownership in any IOM company and receives no kickbacks from the contracted IOM company. Therefore, your RMBSI surgeon has no incentive to inappropriately use IOM during your surgery or try to charge you extra costs irresponsibly. Additionally, the IOM company used by RMBSI has guaranteed to charge reasonable rates within the average national guidelines. You won’t read news articles about any exorbitant charge from our IOM company.
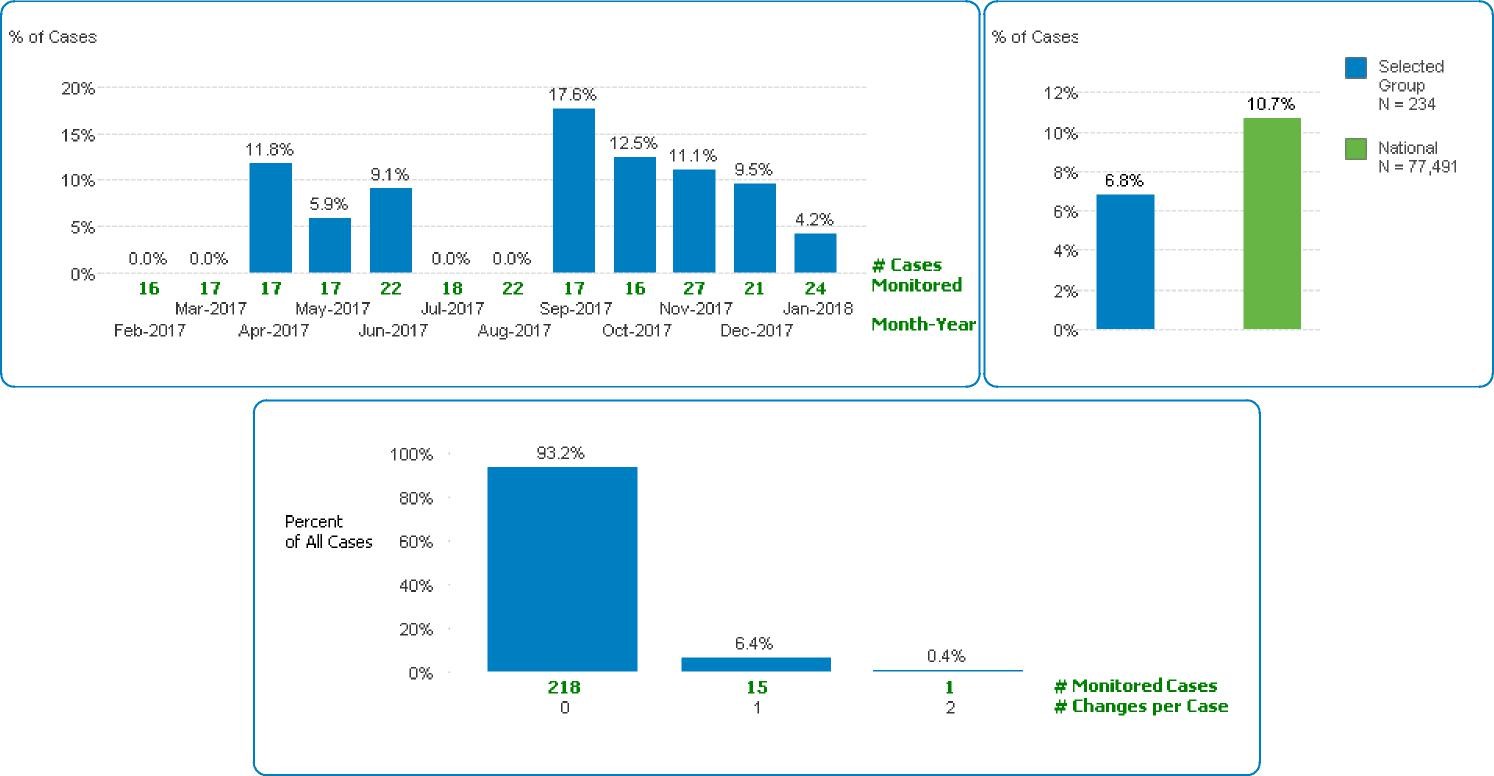
A final and crucial question to discuss with your surgeon is the rate of IOM changes in their surgeries. More than average IOM changes could indicate poor surgical technique and outcomes. Our surgeon at RMBSI has fewer IOM changes than the national average. 234 surgeries over a year period used IOM. 16 cases developed IOM changes, which was 6.8 percent. The national average for IOM changes is approximately 10.7 percent. Seven of these IOM changes were due to surgical positioning, as opposed to a nerve injury during surgery, and all of these IOM changes due to surgical positioning produced no neurologic deficit. Three of these IOM cases were due to anesthesia or low blood pressure. The remaining six cases could be attributable to nerve irritation, and none resulted in permanent postoperative weakness, numbness or pain.
At Rocky Mountain Brain & Spine Institute, we are proud of our minimally invasive techniques and ability to perform surgery with minimal nerve irritation and extraordinarily low complication rates. Contact us today with any questions you may have.





